Advanced Modeling Techniques
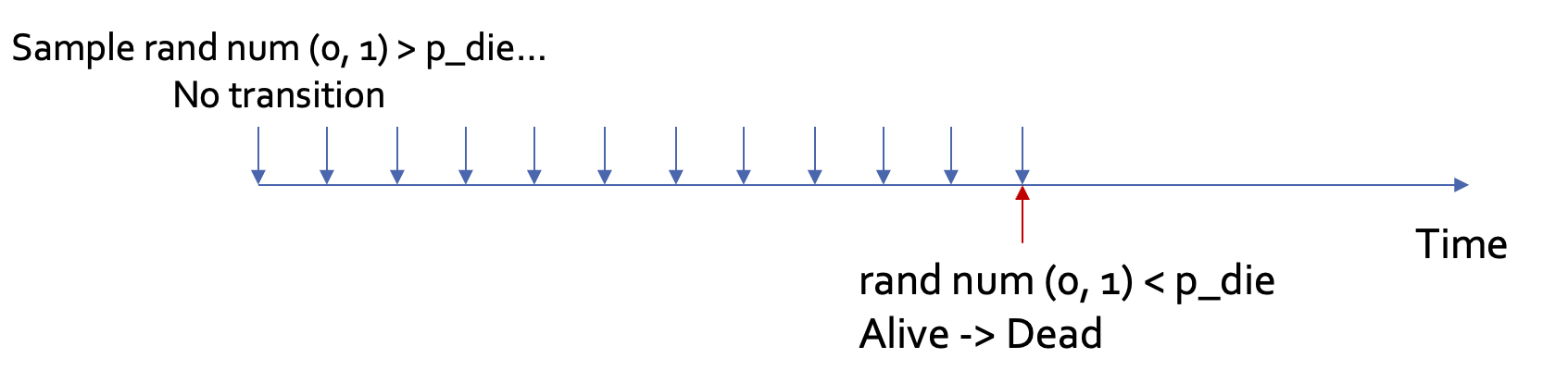
Random numbers
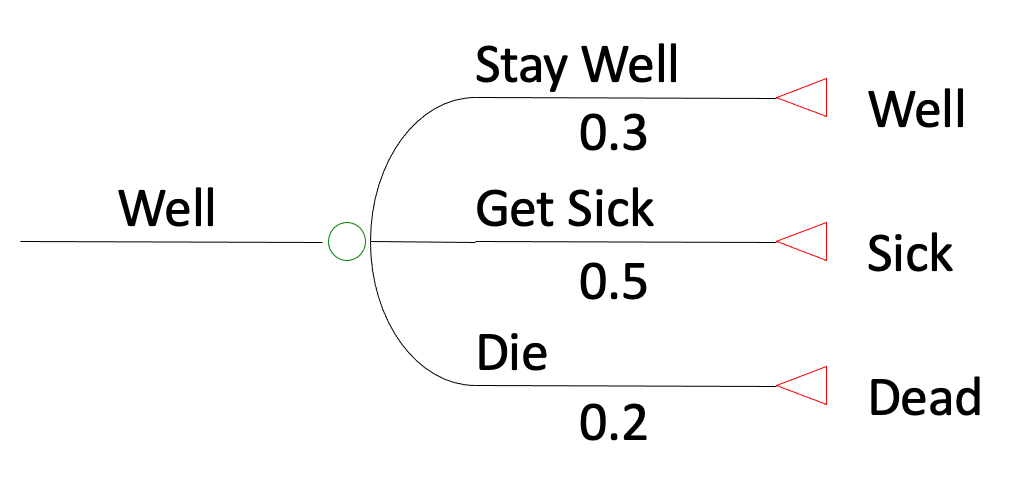
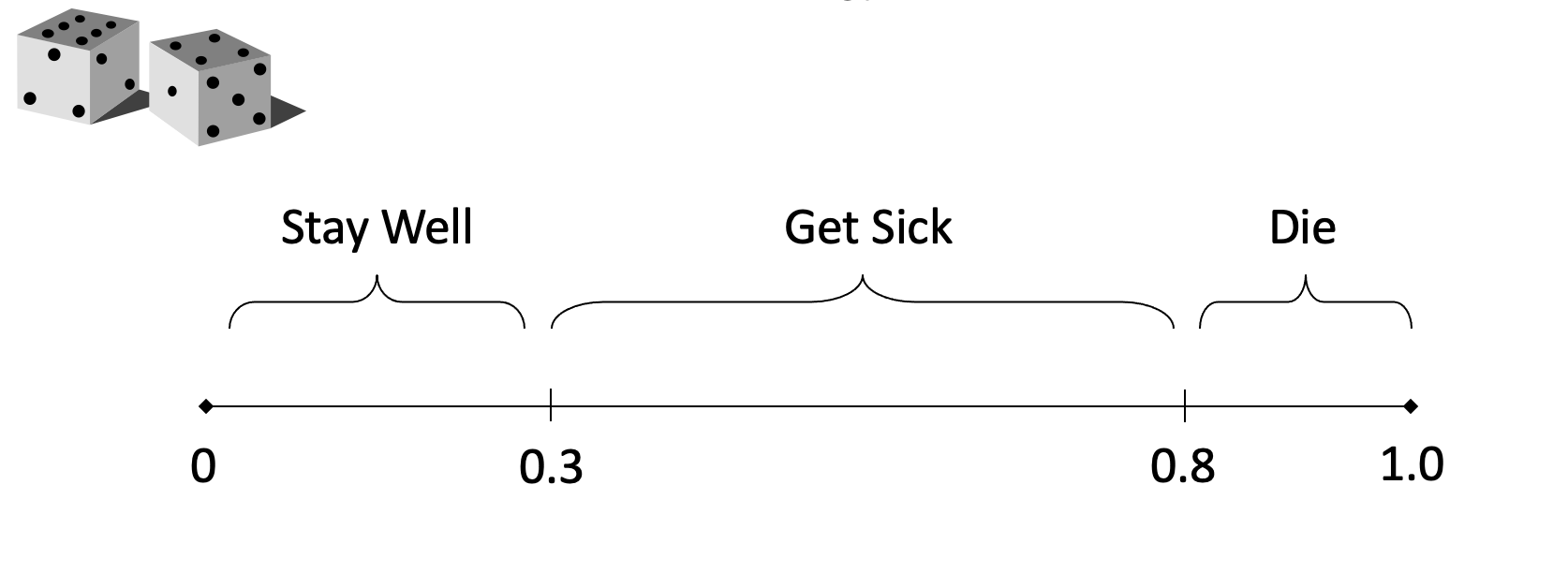
Example
Context: Economic evaluation of TB prevention among people living with HIV in Tanzania
Example
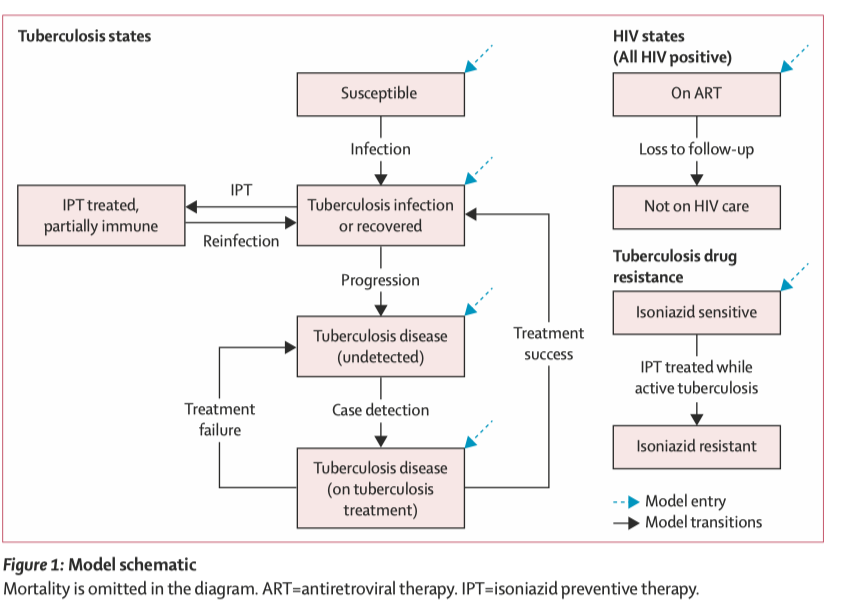
Zhu et al, The Lancet Global Health, 2022
Microsimulation vs DES
Miscrosimulation
Discrete event simulation
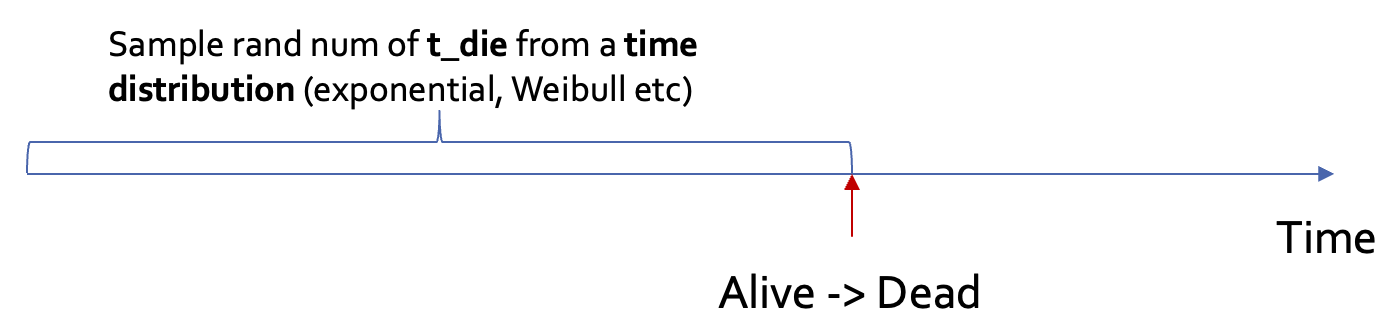
Example
Example
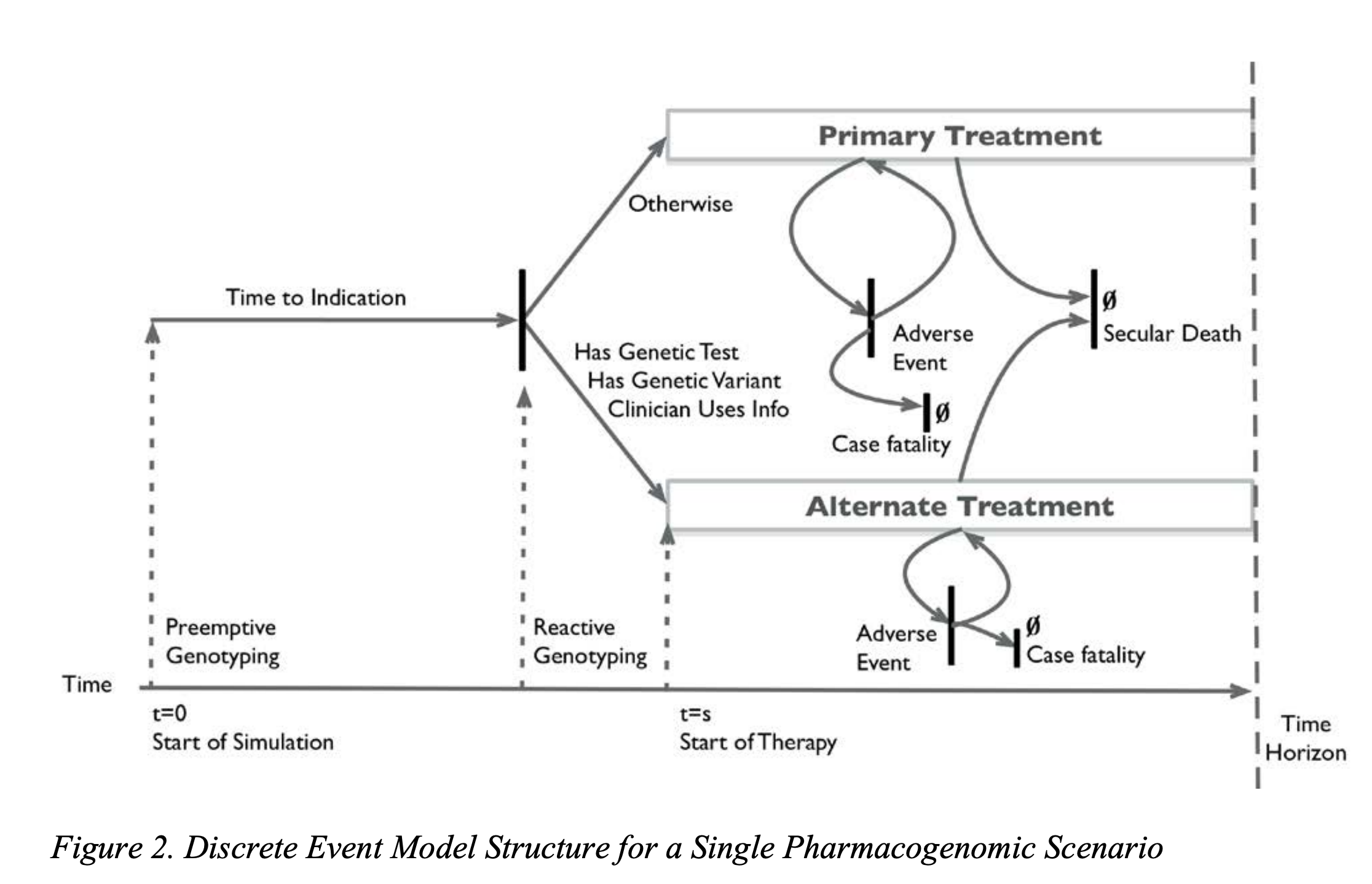
Graves et al, 2017
The SIR model
The most classic model in infectious disease epidemiology. Appropriate for many common infectious diseases (e.g., the flu).
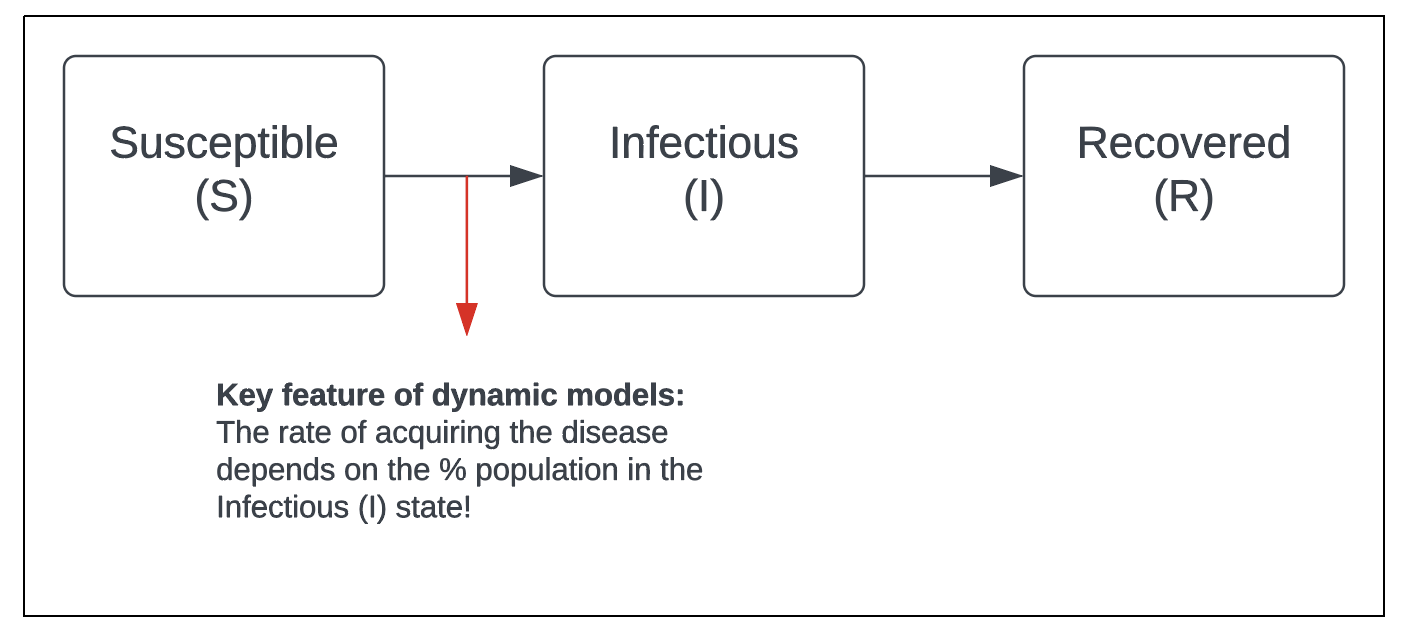
The SIR model
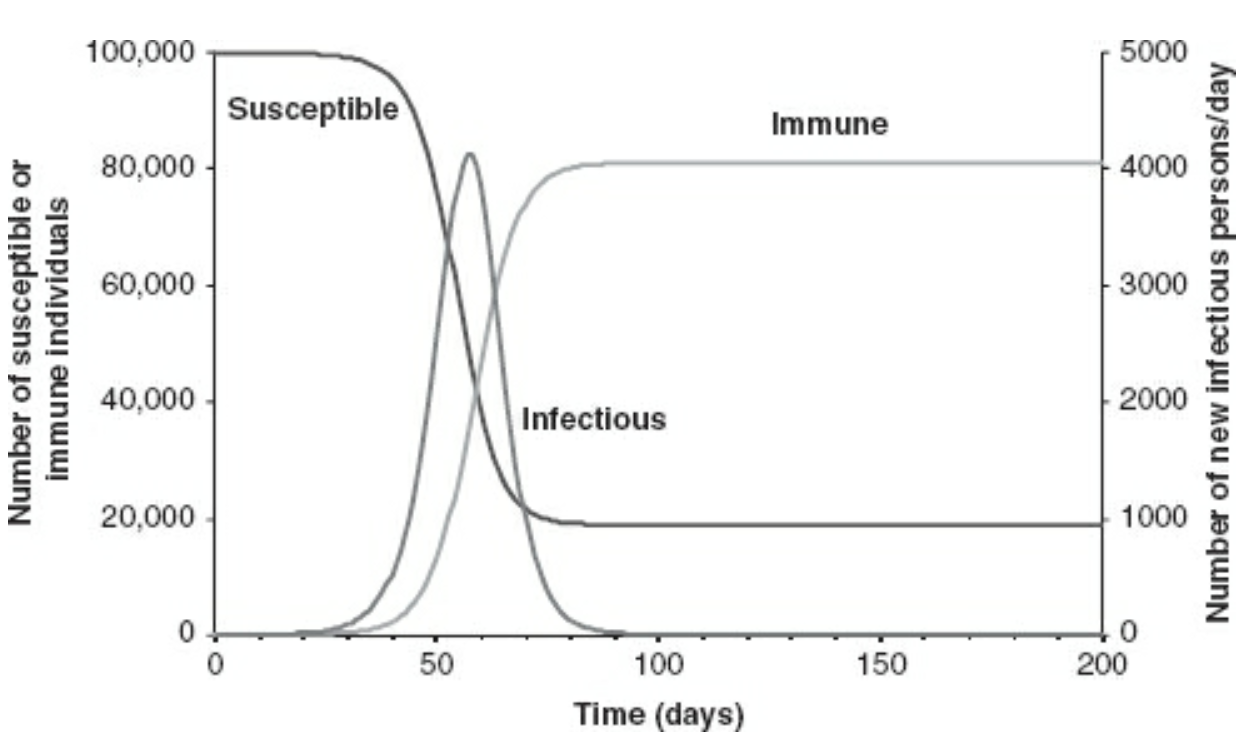
Source: Vynnycky, Emilia; White, Richard. An Introduction to Infectious Disease Modelling.
Variants of the SIR model
From the simple SIR process, we can add more stuctures to reflect the process of a particular disease, for example:
Age- or sex- mixing: appropriate for sexually transmitted diseases
A stage where individuals are infected but not infectious: appropriate for diseases with a latent stage, e.g., TB, COVID-19

Dynamic models are often expressed/solved as difference/differential equations
Example:
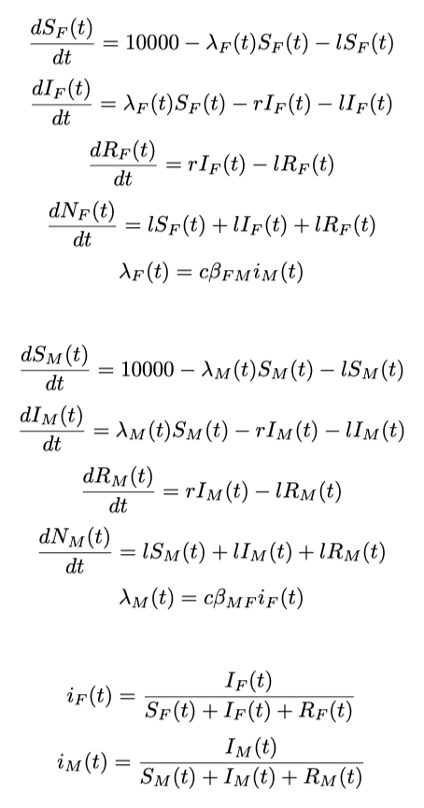
They can be solved by hand or using softwares (e.g. deSolve package in R)
How to choose the right model?
Factors to consider:
Policy question/interventions
Data availability
Natural history of disease
Computational resources available